

A recent lab study has shown that HU-308, a CB2 receptor agonist, is effective in reducing levodopa-induced dyskinesia (LID) in patients with Parkinson’s disease (PD). Larger clinical trials in this area may pave the way for the development of cannabinoid based medicines in the treatment of PD.
What is HU-308?
HU-308 is a synthetic drug that is highly selective for the CB2 receptor; it acts as an agonist at this receptor. An agonist is a substance that produces a physiological response when paired with a receptor.
What is Parkinson’s-Related Levodopa-Induced Dyskinesia (LID)?
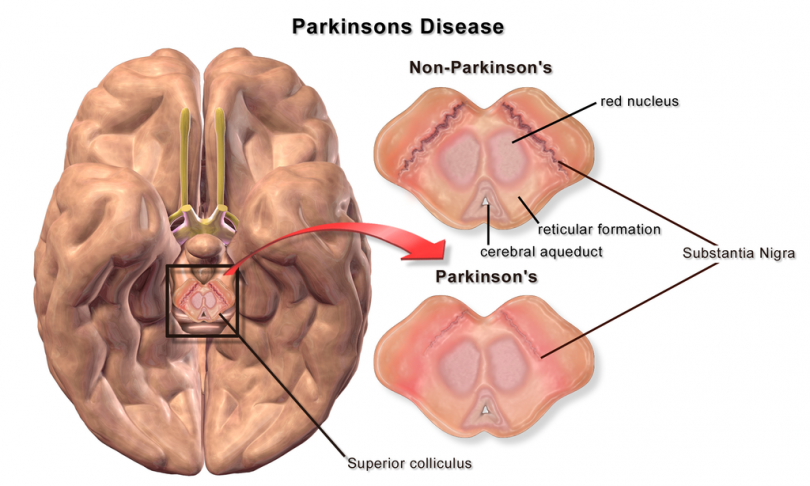
PD is a neurodegenerative disorder that’s associated with the progressive loss of dopaminergic neurons. Loss of dopamine results in locomotor deficits that presents with symptoms such as slowed movement (bradykinesia), slurred speech, rigid muscles, tremors, and poor gait, among others.
Parkinson’s-related LID is a form of dyskinesia (involuntary muscle movements) that results from long-term use of levodopa (L-dopa), an amino acid used in the treatment of Parkinson’s disease. Patients with LID exhibit symptoms such as hyperkinetic movements, chorea, and dystonia.
Dopamine replacement therapy with L-dopa has been used to relieve the motor symptoms associated with PD for many years. Unfortunately, long-term use of L-dopa causes tolerance with over 50% of patients (ages 40–59) developing LID. [1] Once a patient presents with LIDs, L-dopa doses must be reduced and this, in turn, reduces the anti-Parkinsonian efficacy of L-dopa. [1]
The Study
A study published in Neurobiology of Disease in February 2020 investigated the effect of HU-308, a CB2 receptor agonist, on Parkinson-related LIDs. The study was carried out in a lab setting using a mouse model of PD and LIDs. [2]
The results showed that HU-308 was as effective as amantadine, the gold standard treatment for LID, in combating dyskinesia. When combined, the two worked synergistically and produced a greater healing effect. The study also demonstrated that both HU-308 and amantadine decrease “striatal neuroinflammation,” which is responsible for triggering LIDs.
The results from this study warrant further investigation to determine the efficacy of CB2 receptor agonists in treating LID in PD patients. This study also linked altered glial function to the development of LIDs. [2]
HU-308 and Amantadine Therapy for LID
Amantadine is the only drug that has been approved by the FDA for the treatment of LID in patients with PD. The study mentioned above points towards a synergistic effect when HU-308 is combined with amantadine. Given the fact that amantadine has several side effects, combining it with HU-308 may produce more favorable outcomes in patients with Parkinson’s-related LID.
Image Source
https://commons.wikimedia.org/wiki/File:Blausen_0704_ParkinsonsDisease.png (BruceBlaus, CC By 3.0)
References
- Pandey S. et al. “Levodopa-induced Dyskinesia: Clinical Features, Pathophysiology, and Medical Management.” Annals of Indian Academy of Neurology, vol.20, no.3, 2017, pp. 190–198. (Journal Impact Factor 0.891; Cited 32 times)
- Rentsch P. et al. “Targeting the Cannabinoid Receptor CB2 in a Mouse Model of L-dopa induced Dyskinesia.” Neurobiology of Disease, 2020, vol.134, no.104646. (Journal Impact Factor 5.227; Cited 0 times)





